Syndrome of inappropriate antidiuretic hormone (SIADH) causes excessive release of antidiuretic hormone leading to water retention and hyponatremia, while diabetes insipidus results from insufficient antidiuretic hormone activity causing excessive urination and dehydration. SIADH typically presents with low serum sodium and concentrated urine, whereas diabetes insipidus shows high serum sodium levels and dilute urine. Accurate diagnosis and management depend on understanding these contrasting mechanisms affecting fluid balance in pets.
Table of Comparison
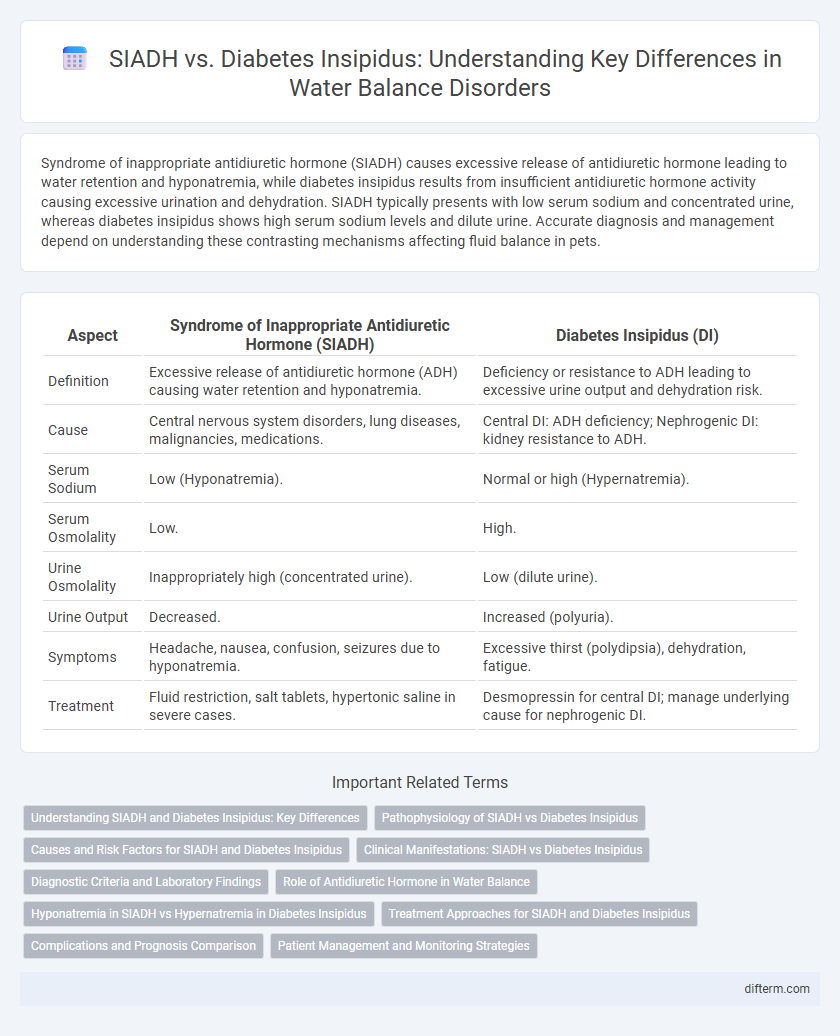
| Aspect | Syndrome of Inappropriate Antidiuretic Hormone (SIADH) | Diabetes Insipidus (DI) |
|---|---|---|
| Definition | Excessive release of antidiuretic hormone (ADH) causing water retention and hyponatremia. | Deficiency or resistance to ADH leading to excessive urine output and dehydration risk. |
| Cause | Central nervous system disorders, lung diseases, malignancies, medications. | Central DI: ADH deficiency; Nephrogenic DI: kidney resistance to ADH. |
| Serum Sodium | Low (Hyponatremia). | Normal or high (Hypernatremia). |
| Serum Osmolality | Low. | High. |
| Urine Osmolality | Inappropriately high (concentrated urine). | Low (dilute urine). |
| Urine Output | Decreased. | Increased (polyuria). |
| Symptoms | Headache, nausea, confusion, seizures due to hyponatremia. | Excessive thirst (polydipsia), dehydration, fatigue. |
| Treatment | Fluid restriction, salt tablets, hypertonic saline in severe cases. | Desmopressin for central DI; manage underlying cause for nephrogenic DI. |
Understanding SIADH and Diabetes Insipidus: Key Differences
Syndrome of inappropriate antidiuretic hormone (SIADH) is characterized by excessive release of antidiuretic hormone (ADH), leading to water retention and hyponatremia, while diabetes insipidus results from insufficient ADH activity, causing excessive urination and dehydration. SIADH often presents with low serum sodium levels and concentrated urine, whereas diabetes insipidus shows high serum sodium and dilute urine due to impaired renal water reabsorption. Accurate diagnosis relies on measuring plasma osmolality, urine osmolality, and ADH levels to distinguish these contrasting disorders affecting fluid balance.
Pathophysiology of SIADH vs Diabetes Insipidus
Syndrome of inappropriate antidiuretic hormone (SIADH) involves excessive release of antidiuretic hormone (ADH), leading to water retention, hyponatremia, and concentrated urine due to increased renal water reabsorption. In contrast, Diabetes Insipidus results from deficient ADH secretion or renal insensitivity to ADH, causing impaired water reabsorption, polyuria, and dilute urine. The distinct pathophysiological mechanisms in SIADH and Diabetes Insipidus directly influence fluid balance and serum sodium concentration.
Causes and Risk Factors for SIADH and Diabetes Insipidus
Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is commonly caused by central nervous system disorders, malignancies, pulmonary diseases, and certain medications leading to excessive release of antidiuretic hormone (ADH). In contrast, Diabetes Insipidus (DI) arises from either insufficient production of ADH (central DI) or renal resistance to ADH (nephrogenic DI), with causes including head trauma, neurosurgery, genetic mutations, lithium use, and chronic kidney disease. Risk factors for SIADH include lung cancers, especially small cell carcinoma, CNS infections, and use of antidepressants, while DI risk factors encompass traumatic brain injury, genetic predisposition, and prolonged hypokalemia or hypercalcemia.
Clinical Manifestations: SIADH vs Diabetes Insipidus
Syndrome of inappropriate antidiuretic hormone (SIADH) presents with hyponatremia, low serum osmolality, concentrated urine, and symptoms such as nausea, headache, and confusion due to water retention and dilutional hyponatremia. Diabetes insipidus is characterized by polyuria, polydipsia, dilute urine with low urine osmolality, hypernatremia, and signs of dehydration caused by insufficient antidiuretic hormone (ADH) activity or renal insensitivity. Distinguishing these conditions clinically is critical as SIADH involves water retention while diabetes insipidus results in excessive water loss.
Diagnostic Criteria and Laboratory Findings
Syndrome of inappropriate antidiuretic hormone (SIADH) is diagnosed by hyponatremia with serum sodium levels typically below 135 mEq/L, low plasma osmolality (<275 mOsm/kg), and inappropriately concentrated urine with urine osmolality >100 mOsm/kg despite hypo-osmolality. In contrast, diabetes insipidus presents with hypernatremia or normal sodium levels, elevated plasma osmolality (>295 mOsm/kg), and dilute urine with urine osmolality usually <300 mOsm/kg, reflecting impaired antidiuretic hormone function or response. Laboratory findings critical for differentiating SIADH from diabetes insipidus include serum sodium, plasma and urine osmolality, and urine sodium concentration, which help guide targeted treatment strategies.
Role of Antidiuretic Hormone in Water Balance
Syndrome of inappropriate antidiuretic hormone (SIADH) causes excessive release of antidiuretic hormone (ADH), leading to water retention and dilutional hyponatremia, whereas diabetes insipidus involves ADH deficiency or insensitivity, resulting in excessive water loss and hypernatremia. ADH regulates water balance by promoting water reabsorption in kidney collecting ducts through aquaporin channels, maintaining plasma osmolality and volume. Disrupted ADH secretion or response directly alters renal water handling, causing distinct fluid and electrolyte imbalances in SIADH versus diabetes insipidus.
Hyponatremia in SIADH vs Hypernatremia in Diabetes Insipidus
Syndrome of inappropriate antidiuretic hormone (SIADH) causes hyponatremia due to excessive release of antidiuretic hormone (ADH), leading to water retention and dilutional low sodium levels. In contrast, diabetes insipidus results in hypernatremia from impaired ADH secretion or renal response, causing excessive water loss and increased serum sodium concentration. Monitoring sodium imbalance is crucial for diagnosing and managing fluid disorders related to ADH dysfunction.
Treatment Approaches for SIADH and Diabetes Insipidus
Treatment for Syndrome of Inappropriate Antidiuretic Hormone (SIADH) primarily involves fluid restriction, administration of hypertonic saline in severe cases, and use of vasopressin receptor antagonists such as tolvaptan to correct hyponatremia. Diabetes insipidus management depends on the type: central diabetes insipidus is treated with desmopressin, a synthetic vasopressin analog, while nephrogenic diabetes insipidus requires addressing underlying causes, maintaining adequate hydration, and use of thiazide diuretics to reduce urine output. Both conditions necessitate careful monitoring of electrolyte levels to prevent complications related to imbalance.
Complications and Prognosis Comparison
Syndrome of inappropriate antidiuretic hormone (SIADH) leads to hyponatremia, causing complications such as seizures, cerebral edema, and altered mental status, with prognosis dependent on early detection and correction of electrolyte imbalance. Diabetes insipidus results in severe polyuria and dehydration, risking hypernatremia, kidney damage, and electrolyte disturbances, where prognosis improves with adequate hormone replacement and fluid management. Both conditions require timely intervention to prevent life-threatening outcomes and long-term organ damage.
Patient Management and Monitoring Strategies
Effective patient management of Syndrome of Inappropriate Antidiuretic Hormone (SIADH) involves fluid restriction, careful electrolyte monitoring, and administration of vasopressin receptor antagonists to correct hyponatremia. In contrast, Diabetes Insipidus requires desmopressin therapy to address antidiuretic hormone deficiency and regular assessment of serum sodium and urine output to prevent dehydration. Both conditions demand ongoing evaluation of fluid balance, with frequent monitoring of weight, urine osmolality, and electrolyte levels to guide treatment adjustments and avoid complications such as seizures or volume overload.
Syndrome of inappropriate antidiuretic hormone (SIADH) vs Diabetes insipidus Infographic