Kwashiorkor and marasmus are severe forms of malnutrition primarily affecting children, characterized by different nutritional deficiencies and clinical signs. Kwashiorkor results from protein deficiency despite adequate calorie intake, leading to edema, an enlarged liver, and skin changes, while marasmus stems from an overall calorie and protein deficiency causing severe wasting and muscle loss without edema. Early diagnosis and appropriate nutritional intervention are crucial for recovery and preventing long-term health complications in affected children.
Table of Comparison
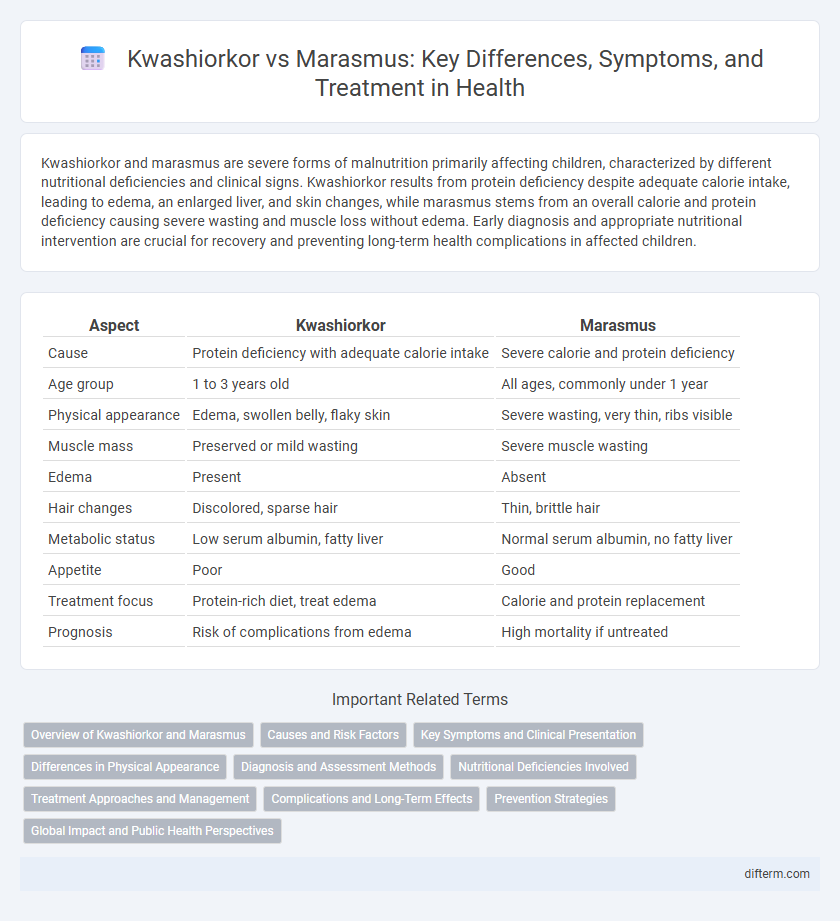
| Aspect | Kwashiorkor | Marasmus |
|---|---|---|
| Cause | Protein deficiency with adequate calorie intake | Severe calorie and protein deficiency |
| Age group | 1 to 3 years old | All ages, commonly under 1 year |
| Physical appearance | Edema, swollen belly, flaky skin | Severe wasting, very thin, ribs visible |
| Muscle mass | Preserved or mild wasting | Severe muscle wasting |
| Edema | Present | Absent |
| Hair changes | Discolored, sparse hair | Thin, brittle hair |
| Metabolic status | Low serum albumin, fatty liver | Normal serum albumin, no fatty liver |
| Appetite | Poor | Good |
| Treatment focus | Protein-rich diet, treat edema | Calorie and protein replacement |
| Prognosis | Risk of complications from edema | High mortality if untreated |
Overview of Kwashiorkor and Marasmus
Kwashiorkor and marasmus are forms of severe malnutrition primarily affecting children in developing countries, with kwashiorkor characterized by protein deficiency leading to edema, an enlarged liver, and skin changes. Marasmus results from a prolonged deficiency of both protein and calories, causing severe wasting, muscle atrophy, and significantly low body weight. Distinguishing factors include kwashiorkor's presence of edema and marasmus's extreme emaciation, critical for appropriate nutritional intervention.
Causes and Risk Factors
Kwashiorkor results primarily from severe protein deficiency despite adequate calorie intake, often occurring in children with sudden weaning from breast milk to a carbohydrate-rich but protein-poor diet. Marasmus is caused by an overall deficiency of calories and nutrients, leading to extreme wasting and muscle loss, commonly seen in cases of prolonged starvation or chronic illness. Risk factors for both conditions include poverty, food insecurity, infections, and lack of access to healthcare in low-resource settings.
Key Symptoms and Clinical Presentation
Kwashiorkor presents with edema, irritability, an enlarged liver, and skin changes such as hyperpigmentation and flaky dermatosis, mainly due to protein deficiency despite adequate calorie intake. Marasmus manifests as severe wasting, muscle atrophy, and loss of subcutaneous fat, reflecting overall calorie deficiency with minimal edema and preserved appetite. Both conditions exhibit signs of malnutrition but differ in the presence of edema and specific skin and liver changes in kwashiorkor versus extreme emaciation in marasmus.
Differences in Physical Appearance
Kwashiorkor is characterized by edema, an enlarged fatty liver, and a distended abdomen, often accompanied by thinning hair and skin depigmentation, while marasmus presents with severe wasting, prominent ribs, and loss of subcutaneous fat, giving a skeletal appearance. In kwashiorkor, muscle mass may be relatively preserved due to fluid retention, contrasting with the extreme muscle wasting seen in marasmus. These distinct physical appearances reflect differences in protein-energy malnutrition and fat depletion between the two conditions.
Diagnosis and Assessment Methods
Kwashiorkor diagnosis primarily relies on clinical signs such as edema, hepatomegaly, and skin changes, supported by biochemical markers like low serum albumin and electrolyte imbalances. Marasmus assessment focuses on severe wasting with significant weight loss and muscle atrophy, often confirmed by anthropometric measurements including weight-for-height and mid-upper arm circumference (MUAC). Laboratory tests for both conditions may include serum protein levels and micronutrient assessments to evaluate the extent of malnutrition and guide treatment plans.
Nutritional Deficiencies Involved
Kwashiorkor primarily results from severe protein deficiency despite adequate calorie intake, leading to edema, fatty liver, and muscle wasting. Marasmus stems from an overall deficiency of both protein and calories, causing significant weight loss, muscle depletion, and energy deficiency. Both conditions indicate malnutrition but differ in the type and severity of nutrient deficits affecting metabolism and growth.
Treatment Approaches and Management
Treatment approaches for kwashiorkor focus on gradual nutritional rehabilitation with therapeutic milk formulas like F75 and F100, correction of electrolyte imbalances, and management of infections due to immune suppression. Marasmus treatment prioritizes caloric repletion with high-energy, nutrient-dense diets to address severe energy deficits, along with careful monitoring of fluid and electrolyte status. Both conditions require individualized medical care, regular follow-up, and supportive interventions to prevent relapse and promote full recovery from severe acute malnutrition.
Complications and Long-Term Effects
Kwashiorkor and marasmus both result in severe malnutrition but differ in complications and long-term effects; kwashiorkor often leads to edema, liver damage, and impaired immune function, increasing susceptibility to infections. Marasmus primarily causes severe wasting, muscle loss, and stunted growth, with long-term effects including delayed cognitive development and weakened physical health. Both conditions can result in irreversible developmental delays and increased childhood mortality if untreated.
Prevention Strategies
Prevention strategies for kwashiorkor and marasmus center on ensuring adequate and balanced nutrition, including sufficient protein and calorie intake, particularly in children under five years old. Promoting exclusive breastfeeding for the first six months and continued breastfeeding alongside appropriate complementary foods helps reduce the risk of malnutrition. Community education programs and food security initiatives play a critical role in preventing these severe forms of protein-energy malnutrition.
Global Impact and Public Health Perspectives
Kwashiorkor and marasmus are severe forms of childhood malnutrition with distinct clinical features but both contribute significantly to global child mortality, particularly in low-income countries. Kwashiorkor, characterized by edema and protein deficiency, affects millions in regions with limited protein access, while marasmus results from severe calorie deficiency, posing widespread risks of muscle wasting and immune suppression. Public health efforts emphasize early detection, nutritional rehabilitation, and sustainable food security programs to reduce incidence and long-term developmental consequences associated with these conditions.
kwashiorkor vs marasmus Infographic