Basal cell carcinoma is the most common type of skin cancer, typically developing in sun-exposed areas and characterized by slow growth and low metastatic potential. In contrast, squamous cell carcinoma tends to be more aggressive, with a higher risk of spreading to other tissues if not treated early. Both require timely medical evaluation and treatment to prevent complications and improve patient outcomes.
Table of Comparison
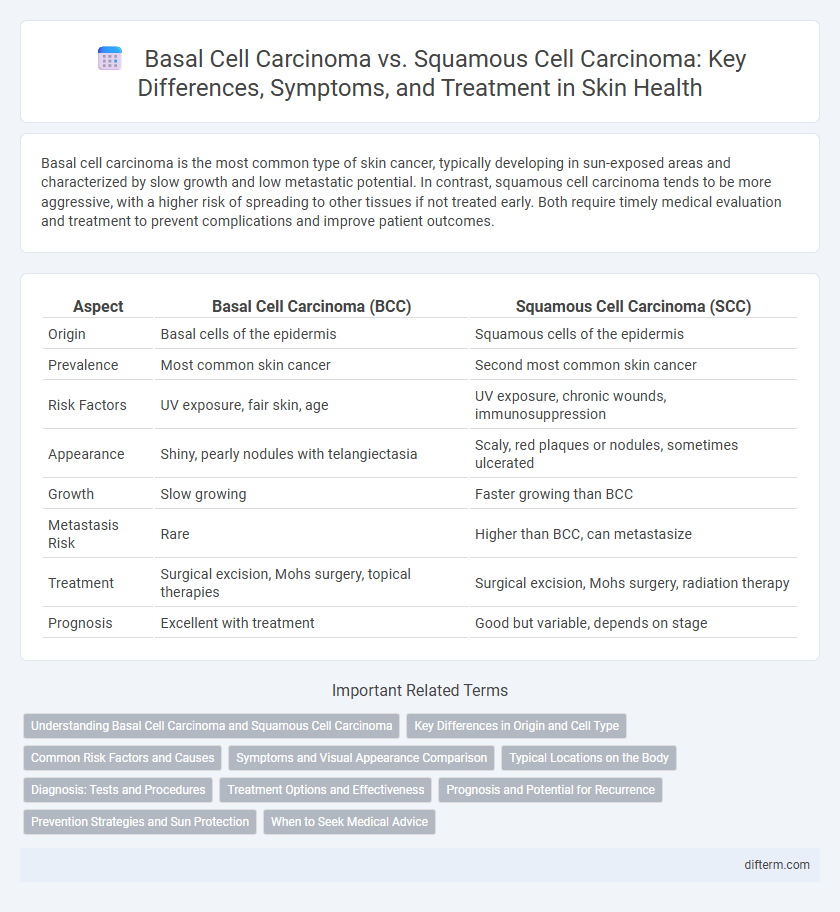
| Aspect | Basal Cell Carcinoma (BCC) | Squamous Cell Carcinoma (SCC) |
|---|---|---|
| Origin | Basal cells of the epidermis | Squamous cells of the epidermis |
| Prevalence | Most common skin cancer | Second most common skin cancer |
| Risk Factors | UV exposure, fair skin, age | UV exposure, chronic wounds, immunosuppression |
| Appearance | Shiny, pearly nodules with telangiectasia | Scaly, red plaques or nodules, sometimes ulcerated |
| Growth | Slow growing | Faster growing than BCC |
| Metastasis Risk | Rare | Higher than BCC, can metastasize |
| Treatment | Surgical excision, Mohs surgery, topical therapies | Surgical excision, Mohs surgery, radiation therapy |
| Prognosis | Excellent with treatment | Good but variable, depends on stage |
Understanding Basal Cell Carcinoma and Squamous Cell Carcinoma
Basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) are the two most common types of non-melanoma skin cancer, each arising from different layers of the epidermis. BCC originates from basal cells in the lower epidermis, characterized by slow growth and rare metastasis, while SCC develops from squamous cells in the upper epidermis and carries a higher risk of spreading to other tissues. Accurate diagnosis and differentiation between BCC and SCC rely on clinical examination and histopathological analysis to guide effective treatment strategies and improve patient outcomes.
Key Differences in Origin and Cell Type
Basal cell carcinoma originates from basal cells in the epidermis, primarily affecting the skin's deepest layer, and is characterized by slow growth and local tissue invasion. Squamous cell carcinoma arises from squamous cells, which are flat, scale-like cells found in the outer layer of the epidermis, often displaying more aggressive behavior and higher metastatic potential. Understanding these differences in cellular origin and histology is crucial for accurate diagnosis, treatment planning, and prognosis in skin cancer management.
Common Risk Factors and Causes
Basal cell carcinoma and squamous cell carcinoma share common risk factors including prolonged exposure to ultraviolet (UV) radiation from the sun or tanning beds, fair skin, a history of sunburns, and immunosuppression. Both types of skin cancer are more prevalent in individuals with a weakened immune system, genetic predispositions, and chronic skin inflammation or exposure to carcinogens such as arsenic. Understanding these overlapping causes is crucial for effective prevention and early detection strategies in high-risk populations.
Symptoms and Visual Appearance Comparison
Basal cell carcinoma typically presents as pearly or waxy bumps with visible blood vessels, often appearing on sun-exposed areas like the face and neck, while squamous cell carcinoma usually manifests as rough, scaly red patches or raised growths that may crust or bleed. The nodules of basal cell carcinoma are generally translucent with a rolled border, contrasting with the firm, crusty texture of squamous cell carcinoma lesions. Both types of skin cancer require early detection, but recognizing the distinct visual and symptomatic differences aids in timely diagnosis and treatment.
Typical Locations on the Body
Basal cell carcinoma typically appears on sun-exposed areas such as the face, especially the nose and forehead, as well as the neck and ears. Squamous cell carcinoma more commonly manifests on the lips, ears, scalp, and dorsal hands, often in regions with chronic sun exposure and previous skin damage. Both types predominantly develop on body sites frequently exposed to ultraviolet radiation, highlighting the importance of sun protection.
Diagnosis: Tests and Procedures
Diagnosis of basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) primarily involves a thorough skin examination followed by a biopsy, such as a punch, shave, or excisional biopsy, to confirm malignancy and determine tumor subtype. Dermoscopy enhances visualization of characteristic features like pearly borders and telangiectasia in BCC, while SCC often displays scaly, crusted lesions with keratinization. Imaging tests, including ultrasound or CT scans, are reserved for advanced cases to assess local invasion or metastasis, especially in high-risk SCC.
Treatment Options and Effectiveness
Basal cell carcinoma (BCC) treatment primarily involves surgical excision, Mohs micrographic surgery, and topical therapies like imiquimod, which offer high cure rates exceeding 95%. Squamous cell carcinoma (SCC) often requires more aggressive management, including wide local excision, radiation therapy, and sometimes systemic treatments for advanced stages, with cure rates varying by tumor size and invasion depth. Early detection and tailored treatment plans significantly improve outcomes and reduce recurrence risks for both skin cancers.
Prognosis and Potential for Recurrence
Basal cell carcinoma (BCC) generally has an excellent prognosis with a low potential for recurrence when treated early, often exhibiting slow growth and minimal metastasis risk. In contrast, squamous cell carcinoma (SCC) presents a higher risk of recurrence and metastasis, especially if poorly differentiated or located on high-risk sites such as the lips or ears. Close monitoring and timely treatment are critical for SCC due to its more aggressive nature and propensity for local tissue invasion and spread.
Prevention Strategies and Sun Protection
Basal cell carcinoma and squamous cell carcinoma risk can be significantly reduced through rigorous sun protection strategies, including consistent use of broad-spectrum sunscreen with SPF 30 or higher, wearing protective clothing, and seeking shade during peak UV radiation hours. Avoiding tanning beds and limiting direct sun exposure are critical preventive measures recommended by dermatological experts to decrease carcinogenic UV damage to the skin. Regular skin examinations for early detection further enhance preventive efforts, particularly in individuals with fair skin, outdoor occupations, or a history of sunburns.
When to Seek Medical Advice
Any persistent sore, lump, or scaly patch on the skin that does not heal within a few weeks should prompt immediate medical evaluation to rule out basal cell carcinoma or squamous cell carcinoma. Rapidly growing lesions, changes in color or texture, pain, bleeding, or ulceration are key warning signs that necessitate prompt consultation with a dermatologist. Early diagnosis significantly improves treatment outcomes for these common types of non-melanoma skin cancer.
Basal cell carcinoma vs Squamous cell carcinoma Infographic