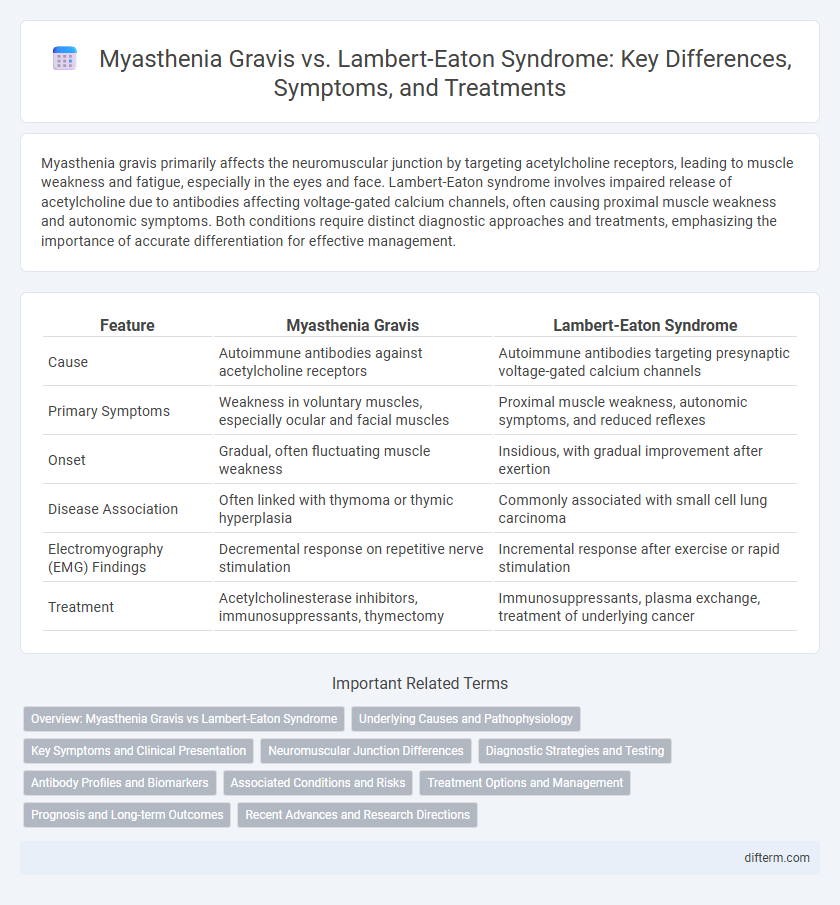
Myasthenia gravis primarily affects the neuromuscular junction by targeting acetylcholine receptors, leading to muscle weakness and fatigue, especially in the eyes and face. Lambert-Eaton syndrome involves impaired release of acetylcholine due to antibodies affecting voltage-gated calcium channels, often causing proximal muscle weakness and autonomic symptoms. Both conditions require distinct diagnostic approaches and treatments, emphasizing the importance of accurate differentiation for effective management.
Table of Comparison
| Feature | Myasthenia Gravis | Lambert-Eaton Syndrome |
|---|---|---|
| Cause | Autoimmune antibodies against acetylcholine receptors | Autoimmune antibodies targeting presynaptic voltage-gated calcium channels |
| Primary Symptoms | Weakness in voluntary muscles, especially ocular and facial muscles | Proximal muscle weakness, autonomic symptoms, and reduced reflexes |
| Onset | Gradual, often fluctuating muscle weakness | Insidious, with gradual improvement after exertion |
| Disease Association | Often linked with thymoma or thymic hyperplasia | Commonly associated with small cell lung carcinoma |
| Electromyography (EMG) Findings | Decremental response on repetitive nerve stimulation | Incremental response after exercise or rapid stimulation |
| Treatment | Acetylcholinesterase inhibitors, immunosuppressants, thymectomy | Immunosuppressants, plasma exchange, treatment of underlying cancer |
Overview: Myasthenia Gravis vs Lambert-Eaton Syndrome
Myasthenia gravis is an autoimmune neuromuscular disorder characterized by antibodies targeting acetylcholine receptors, leading to muscle weakness and fatigue primarily in the eyes, face, and limbs. Lambert-Eaton syndrome involves autoantibodies against presynaptic voltage-gated calcium channels, causing impaired acetylcholine release and proximal muscle weakness often associated with malignancies like small-cell lung cancer. Differentiating these disorders relies on clinical presentation, antibody testing, and electrophysiological studies, emphasizing distinct pathophysiological mechanisms and therapeutic interventions.
Underlying Causes and Pathophysiology
Myasthenia gravis is an autoimmune disorder characterized by antibodies targeting acetylcholine receptors at the neuromuscular junction, leading to impaired signal transmission and muscle weakness. Lambert-Eaton syndrome involves autoantibodies against presynaptic voltage-gated calcium channels, reducing acetylcholine release and causing proximal muscle weakness. Both disorders disrupt neuromuscular communication through distinct mechanisms affecting synaptic transmission and exhibit varying associations with malignancies such as thymoma in myasthenia gravis and small cell lung cancer in Lambert-Eaton syndrome.
Key Symptoms and Clinical Presentation
Myasthenia gravis primarily presents with fluctuating muscle weakness, especially affecting the ocular muscles, resulting in ptosis and diplopia, while Lambert-Eaton syndrome is characterized by proximal muscle weakness that improves with activity and autonomic symptoms like dry mouth. In myasthenia gravis, muscle weakness worsens with exertion and improves with rest, whereas Lambert-Eaton syndrome exhibits reduced or absent deep tendon reflexes and facilitation of muscle strength after repeated use. Both disorders involve impaired neuromuscular transmission but differ in their underlying pathophysiology and clinical manifestations, guiding diagnostic and therapeutic strategies.
Neuromuscular Junction Differences
Myasthenia gravis primarily involves antibodies targeting acetylcholine receptors at the neuromuscular junction, leading to impaired signal transmission and muscle weakness. Lambert-Eaton syndrome features antibodies against voltage-gated calcium channels on presynaptic nerve terminals, reducing acetylcholine release and causing diminished muscle activation. These distinct pathogenic mechanisms result in different clinical presentations and responses to treatment in neuromuscular disorders.
Diagnostic Strategies and Testing
Myasthenia gravis diagnosis primarily relies on the detection of acetylcholine receptor antibodies and electrophysiological tests such as repetitive nerve stimulation and single-fiber electromyography to assess neuromuscular transmission. Lambert-Eaton syndrome diagnosis emphasizes voltage-gated calcium channel antibody testing and characteristic electrophysiological findings like incremental response to high-frequency repetitive nerve stimulation. Imaging studies, including CT or MRI scans, are crucial in Lambert-Eaton syndrome for identifying underlying malignancies, particularly small cell lung cancer.
Antibody Profiles and Biomarkers
Myasthenia gravis primarily involves antibodies against acetylcholine receptors (AChR) or muscle-specific kinase (MuSK), serving as key biomarkers for diagnosis. Lambert-Eaton syndrome is characterized by antibodies targeting presynaptic P/Q-type voltage-gated calcium channels (VGCC), which disrupt neurotransmitter release and are critical for its identification. Differentiating these distinct antibody profiles facilitates accurate diagnosis and guides targeted immunotherapy in neuromuscular junction disorders.
Associated Conditions and Risks
Myasthenia gravis is frequently linked with autoimmune disorders such as thyroid disease and rheumatoid arthritis, carrying risks of respiratory failure during severe muscle weakness episodes. Lambert-Eaton syndrome often associates with malignancies, particularly small cell lung cancer, increasing the risk of paraneoplastic complications. Both conditions pose risks of progressive muscle weakness, but underlying cancer presence in Lambert-Eaton syndrome significantly influences prognosis and treatment strategies.
Treatment Options and Management
Myasthenia gravis treatment primarily involves acetylcholinesterase inhibitors like pyridostigmine, immunosuppressants, and thymectomy to improve neuromuscular transmission and reduce antibody production. Lambert-Eaton syndrome management focuses on medications such as amifampridine to enhance acetylcholine release and immunotherapies like corticosteroids or plasmapheresis to decrease autoantibodies targeting voltage-gated calcium channels. Both conditions benefit from symptomatic treatment and immunomodulation, but Lambert-Eaton syndrome often requires management of underlying malignancies, particularly small cell lung cancer.
Prognosis and Long-term Outcomes
Myasthenia gravis typically presents with a favorable prognosis when managed with immunosuppressive therapies and acetylcholinesterase inhibitors, often allowing patients to achieve near-normal muscle strength and prolonged survival. Lambert-Eaton syndrome, although rarer and frequently associated with underlying malignancies such as small cell lung cancer, shows improvement in muscle strength with treatment of both the neuromuscular disorder and the cancer, but long-term outcomes depend heavily on cancer prognosis. Both conditions require ongoing medical management and monitoring to optimize quality of life and prevent complications from muscle weakness.
Recent Advances and Research Directions
Recent advances in Myasthenia Gravis research highlight novel immunotherapies targeting acetylcholine receptor antibodies, improving symptom management and reducing relapse rates. Investigations into Lambert-Eaton Syndrome focus on enhancing voltage-gated calcium channel function and developing biomarkers for early diagnosis, aiding personalized treatment strategies. Ongoing studies emphasize the genetic and immunological differences between these neuromuscular disorders to optimize drug development and therapeutic outcomes.
Myasthenia gravis vs Lambert-Eaton syndrome Infographic